At Blue Bird Day, we often suggest exploring AAC options for our clients. However, many caretakers are resistant to this suggestion. Clinicians often hear: “But our child uses words,” or “We want our child to speak.” Blue Bird’s Speech-Language Pathologists are here to address common concerns about AAC.
What is AAC?
AAC is an acronym for Augmentative and Alternative Communication. It is any form of communication except oral speech. AAC can be high-tech, speech-generating devices (SGDs) such as the TouchChat App that many BBD clients use on an iPad. It can also be low-tech, such as a static communication board made of pictures the child touches to communicate. An example is shown below:
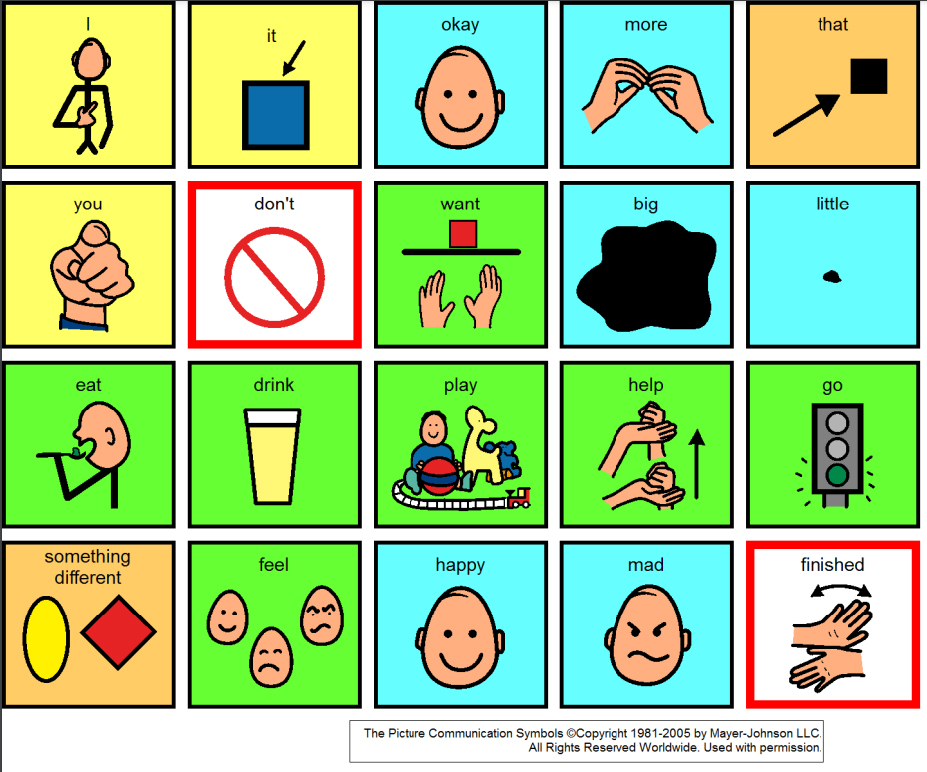
The key words to remember when thinking about AAC are “augmentative” and “alternative.” AAC augments, or adds to, the user’s communication skills. AAC offers an alternative, additional choice for users to communicate. It does not replace a child’s current forms of communication, such as verbalizations, signs, and body language.
Common Myths about AAC
1. AAC will prevent my child from talking.
Using AAC will not prevent or delay a child from using verbal speech, nor will it decrease verbal communication. Evidence indicates that interventions incorporating the use of AAC increase speech production (Aftab et al, 2023; Miller, 2006). Use of speech generating devices, in particular, can aid in overall language development and increase independence (Aftab et al, 2023).
2. AAC is expensive.
Low-tech AAC, such as a picture board, can be quickly made by BBD teachers. These boards are easily customizable for each child and for different activities. High-tech options are often covered by health insurance, or can be obtained for trial purposes from various “lending libraries” operated by non-profits and state and federal agencies.
3. A high-tech device will increase my child’s screen time, and I want to decrease screen time.
The American Academy of Pediatrics (AAP) recommends no screen time at all for children, except for video chatting, until 18-24 months of age. The AAP recommends less than one hour of screen time per day for children ages 2-5 years. High-tech AAC devices typically have a
“guided access” setting, which prevents the child from navigating away from the AAC system. It is recommended that an iPad (or other device) used for AAC be used exclusively for communication. Children (and adults) should not access the internet or other apps or features from a dedicated AAC device. Because high-tech AAC devices are used actively and for communication, they are generally excluded from the definition of “screen time.”
Conclusion
The world of AAC can be overwhelming and confusing. If AAC is suggested for your child, or if you are interested in learning more about AAC, please reach out to the Blue Bird Day speech therapy team.
Further Information and Resources
https://www.asha.org/public/speech/disorders/aac/
https://www.bostonabilitycenter.com/post/aac-myths-and-facts
https://praacticalaac.org/
https://aaccommunity.net/2017/11/start-with-a-little-or-a-lot-introducing-core-boards/
References
Aftab, A., Chhavi Arora Sehgal, Noohu, M. M., & Jaleel, G. (2023). Clinical Effectiveness of AAC Intervention in Minimally Verbal Children With ASD: A Systematic Review. NeuroRegulation, 10(4), 239–252. https://doi.org/10.15540/nr.10.4.239
Millar, D. C., Light, J. C., & Schlosser, R. W. (2006). The impact of augmentative and alternative communication intervention on the speech production of individuals with developmental disabilities: A research review. Journal of Speech, Language, and Hearing Research, 49(2), 248–264. https://doi.org/10.1044/1092-4388(2006/021)
“Tips for Setting Screen Time Limits as a Parent.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 10 Feb. 2022, www.mayoclinic.org/healthy-lifestyle/childrens-health/in-depth/screen-time/art-20047952.

Blue Bird Day—the first therapeutic preschool and kindergarten program in the nation—fosters socialization, sensory regulation, and pre-academic learning in children ages 2-6 years. Our compassionate therapists practice a relationship-based and family-centered approach, provide parent training, and collaborate on goals and individualized intensive treatment plans for your child.
We believe in a collaborative and multi-disciplinary team approach to therapy. A team of occupational therapists, speech-language pathologists, dietitians, developmental therapists, behavioral therapists, physical therapists, and therapeutic assistants are created for each child to ensure child and family are fully supported and the best possible results are achieved.
Options for individualized, group and virtual therapy sessions are available as well.
Want to learn more or you have a specific question? Feel free to connect with us here!


{kind=link}
{kind=link}
{kind=link}